You’re not “bad at sleep”—you might be solving the wrong problem
You do the “right” things: you get in bed on time, you log 7–9 hours, you even cut caffeine. Then morning still feels like you barely slept, or your partner reports things you can’t explain—snoring, pauses in breathing, kicking, shouting, wandering.
When that happens, pushing harder on insomnia advice can waste weeks. If the issue is breathing, a body clock that won’t line up, or sudden sleepiness that hits at unsafe times, more relaxation apps won’t fix it.
If you’re getting 7–9 hours, what does “unrefreshed” actually look like?
That “unrefreshed” feeling usually shows up as a mismatch: the clock says you slept enough, but your body acts like you didn’t. You might wake with a heavy head, dry mouth, or a dull headache. You might need a long “warm-up” to think clearly, or feel irritable for no clear reason. Some people can do the basics but can’t sustain attention—reading the same paragraph twice, missing turns while driving, or feeling strangely clumsy until late morning.
A useful clue is how quickly sleepiness returns after you’re up. If you’re yawning hard by mid-morning, falling asleep in meetings, or needing naps that still don’t reset you, it points away from “just stress.” If weekends don’t help, or you wake up feeling worse after a full night, track two weeks: bedtime, wake time, naps, morning symptoms, and any snoring or gasping your partner notices.
That record makes the next question clearer: is your sleep being disrupted by breathing, movement, timing, or something neurologic?
Snoring, gasping, dry mouth: when it’s more than ‘annoying noise’

Breathing issues are often the easiest to miss because you’re asleep for the worst part. A partner hears loud snoring, then a quiet stretch, then a snort or gasp. You wake up with a dry mouth, a sore throat, or a morning headache and assume it’s “just how you sleep.” But those stop-start patterns can keep pulling you into lighter sleep, so the clock shows 8 hours while your brain never gets steady, deep rest.
A few practical red flags: your partner notices pauses in breathing, you wake up choking or with your heart racing, you’re a habitual mouth-breather at night, or you get up to pee multiple times without a clear reason. Daytime clues matter too—nodding off while reading, in traffic, or after lunch even when you “slept enough.”
Home sleep tests can miss some cases, and in-lab studies take scheduling and money. Still, if gasping or witnessed pauses show up, it’s reasonable to ask your clinician about sleep apnea screening and bring that two-week log.
Do you nod off at the wrong time—or feel dragged under by sleep attacks?
That daytime nodding off matters because it’s not always “I’m tired.” Sometimes it feels sudden and out of proportion to your night: you’re mid-conversation, reading to a kid, or stopped at a red light and you get pulled toward sleep like a switch flipped.
If you can’t stay awake in low-stimulation situations (meetings, lectures, passenger seat) even after 7–9 hours, note what else comes with it. Do short naps feel unusually refreshing? Do you have brief moments of muscle weakness with laughter or surprise, like your knees buckling or your head dropping? Do you get vivid dream-like images as you fall asleep or wake, or wake unable to move for a few seconds? Those clusters are worth bringing up directly, because they point beyond “bad sleep hygiene.”
A two-week sleep log plus a clinician visit can tell you whether a sleep specialist or targeted testing makes sense—especially before this shows up behind the wheel.
The nights your legs won’t cooperate (or your partner says you kick)
That same two-week log can reveal a different kind of disruption: you get to bed tired, but the moment you try to get comfortable, your legs demand movement. People describe it as an urge to move, crawling or tingling sensations, or a feeling that builds until you stretch, pace, or rub your calves. If the pattern is worse at night, improves with movement, and keeps delaying sleep, it can fit restless legs syndrome—especially if it flares with low iron, kidney disease, or certain antidepressants.
Sometimes you don’t feel an urge at all, but a partner reports repetitive kicking or twitching every 20–40 seconds. That can fragment sleep without fully waking you. Practical next steps: track evenings when symptoms hit, caffeine, and any new meds; ask your clinician about ferritin/iron testing. The frustrating part is that “normal” iron labs can still miss it, and treatment often takes a few tries. If the pattern persists, bring the log and ask whether a sleep study is warranted—especially before blaming your schedule.
When your sleep schedule keeps ‘resetting’ no matter how hard you try
Before blaming your schedule, notice if your “insomnia” is really timing. A common pattern is that you can sleep well—just not at the hours you want. You aim for 10:30 p.m., lie there wide awake, finally sleep at 1–2 a.m., then feel wrecked for a 7 a.m. alarm. On weekends, you drift later, sleep in, and Monday feels like jet lag.
If that’s you, think body clock, not willpower. Delayed sleep phase is the classic version: late sleepiness, late wake-ups, and trouble shifting earlier even with good habits. Night shifts, early school drop-offs, and evening light from screens can lock it in. The real-world problem is consistency—kids, commuting, and late meetings make “same wake time daily” hard, and bright-light timing or melatonin can backfire if you guess.
Track sleep and light exposure for two weeks, then bring it up—especially if odd behaviors show up when you finally do fall asleep.
Acting out dreams, sleepwalking, night terrors—how weird is too weird?
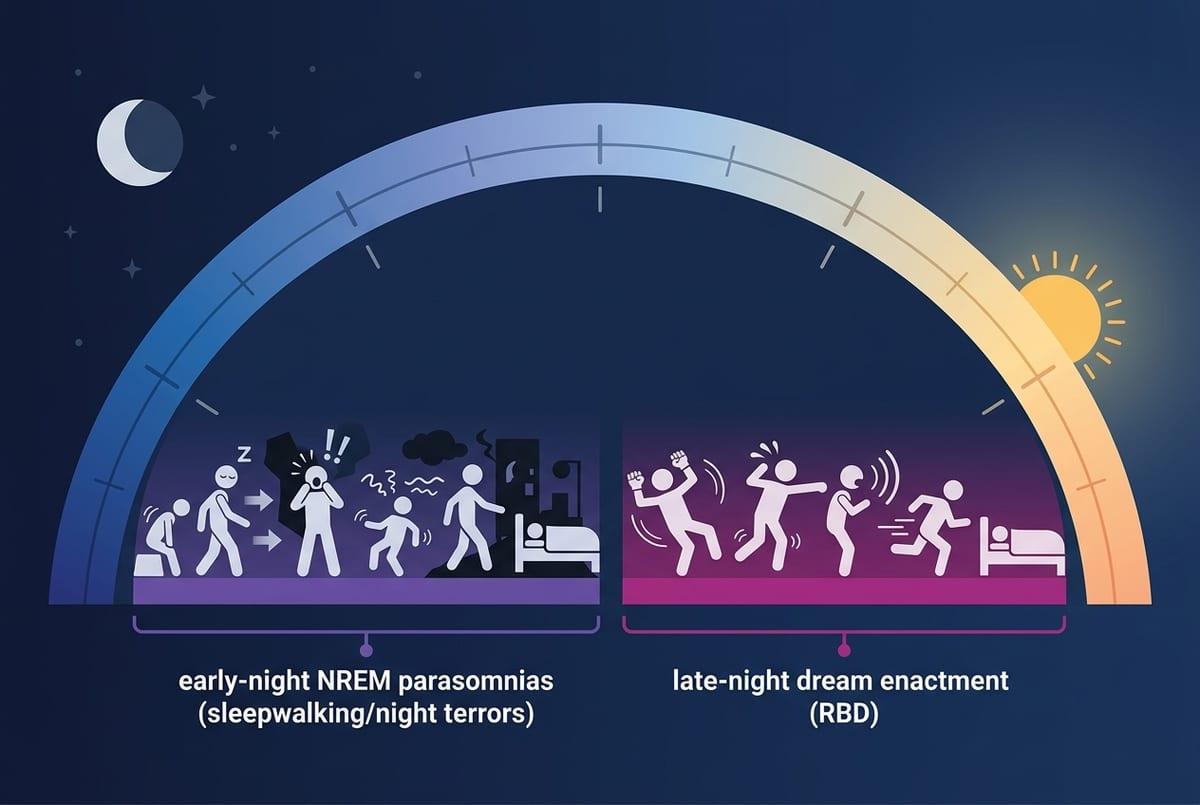
Odd behaviors can range from harmless to risky, and the difference is often what your body is doing, not how “embarrassing” it sounds. If you sit up, mumble, or wander with a blank, hard-to-wake look, it often happens in the first third of the night. People may have no memory of it in the morning. Night terrors can look intense—screaming, pounding heart, sweating—yet the person stays confused rather than fully awake.
Acting out dreams is a different pattern: punching, kicking, or shouting in a way that seems to match a dream, more often later in the night. That’s a safety issue if anyone shares the bed. New episodes after starting or stopping certain meds, or after sleep deprivation also matter because they can trigger or worsen these events.
It’s hard to describe what you never witnessed. If it’s happening, take a short phone video (safely), note timing, injuries, and med changes, then use that to choose a next step without guessing a diagnosis.
Choosing a sensible next step without spiraling into self-diagnosis
That short phone video or two-week log is your anchor when your brain wants to jump to a diagnosis. Bring it to a primary care visit and ask a plain question: “Which pattern does this look most like—breathing, movement, timing, or neurologic—and what test fits?” If there’s gasping, witnessed pauses, or dozing while driving, treat it as time-sensitive and ask about sleep apnea screening or a sleep specialist referral.
If symptoms are annoying but not dangerous, pick one trackable change for two weeks (caffeine cutoff, consistent wake time) so you’re not changing everything at once. The downside is cost and waitlists, so go in with your data and a specific ask: home test vs in-lab study, ferritin/iron labs, or circadian guidance.